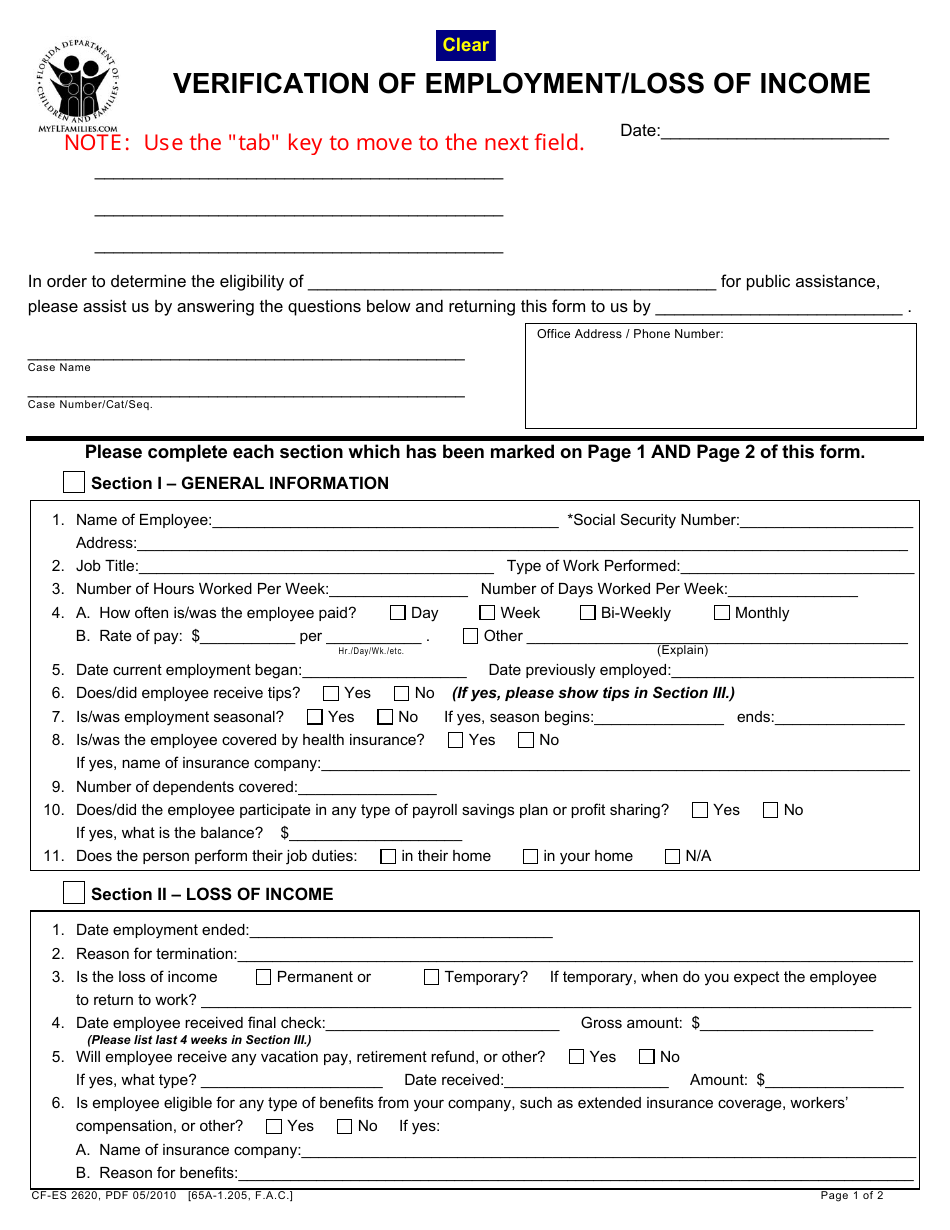
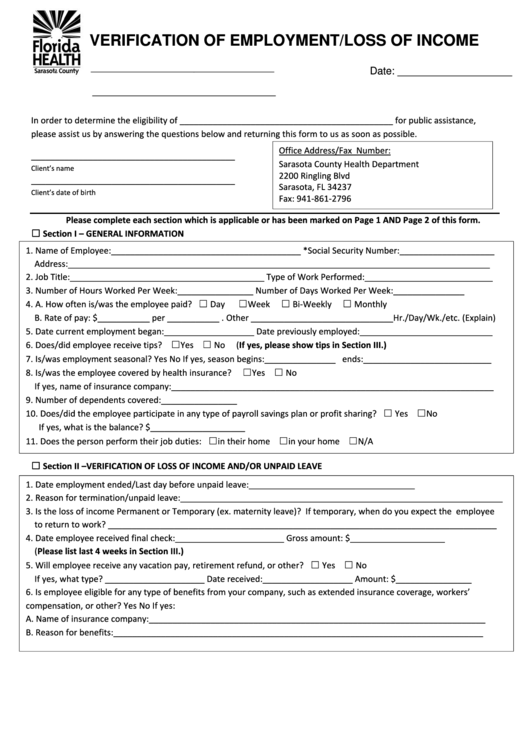
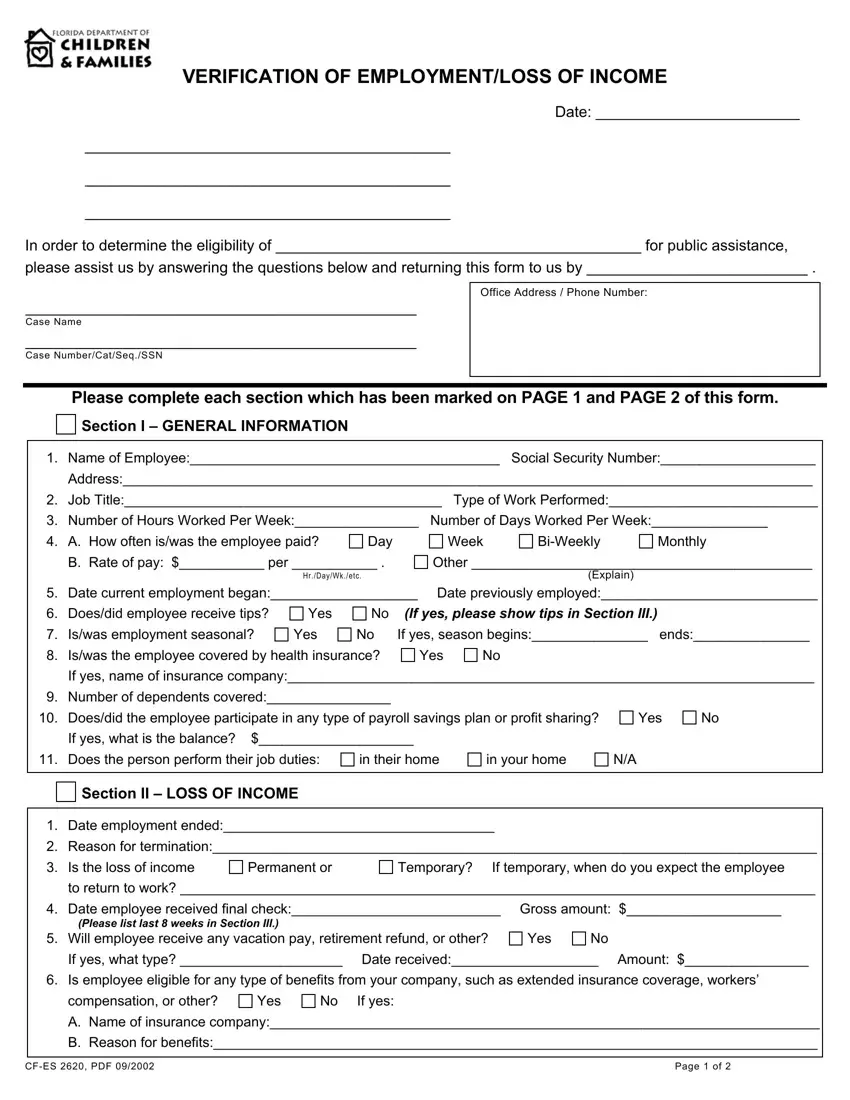
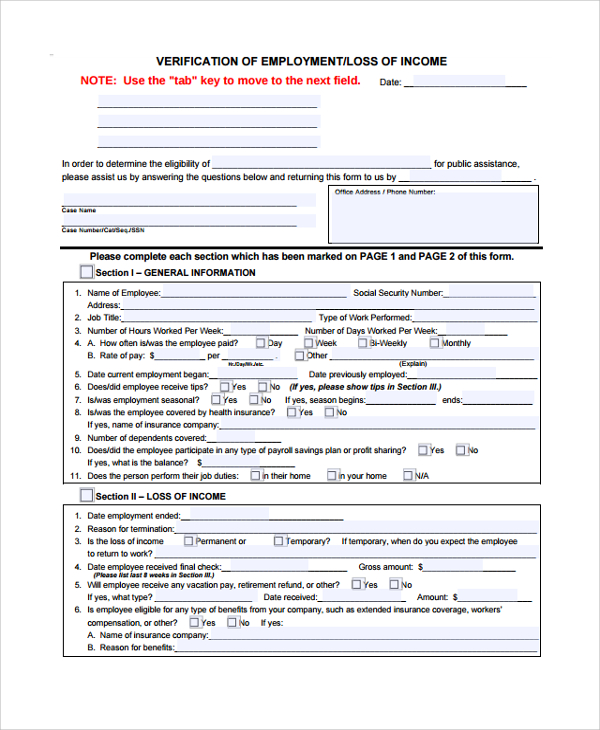
Employment Verification Loss Of Income Form - In order to determine the eligibility of ___________________________________________ for public assistance, please assist us by. Complete this section only if you are reporting a loss of income. If hours/rate of pay has varied, please explain. Verification of employment/loss of income in order to determine the eligibility of _____________________________________________. Date employment ended | fecha que el empleo terminó?
Verification of employment/loss of income in order to determine the eligibility of _____________________________________________. If hours/rate of pay has varied, please explain. Date employment ended | fecha que el empleo terminó? In order to determine the eligibility of ___________________________________________ for public assistance, please assist us by. Complete this section only if you are reporting a loss of income.
Verification of employment/loss of income in order to determine the eligibility of _____________________________________________. Date employment ended | fecha que el empleo terminó? In order to determine the eligibility of ___________________________________________ for public assistance, please assist us by. Complete this section only if you are reporting a loss of income. If hours/rate of pay has varied, please explain.
Form CFES2620 Fill Out, Sign Online and Download Fillable PDF
Date employment ended | fecha que el empleo terminó? Complete this section only if you are reporting a loss of income. In order to determine the eligibility of ___________________________________________ for public assistance, please assist us by. If hours/rate of pay has varied, please explain. Verification of employment/loss of income in order to determine the eligibility of _____________________________________________.
Free Printable Loss Of Wages Form Printable Forms Free Online
Complete this section only if you are reporting a loss of income. In order to determine the eligibility of ___________________________________________ for public assistance, please assist us by. Date employment ended | fecha que el empleo terminó? If hours/rate of pay has varied, please explain. Verification of employment/loss of income in order to determine the eligibility of _____________________________________________.
Verification Of Employment/loss Of Form printable pdf download
Date employment ended | fecha que el empleo terminó? Verification of employment/loss of income in order to determine the eligibility of _____________________________________________. In order to determine the eligibility of ___________________________________________ for public assistance, please assist us by. Complete this section only if you are reporting a loss of income. If hours/rate of pay has varied, please explain.
40+ Verification Letter Samples (& Proof of Letters)
Verification of employment/loss of income in order to determine the eligibility of _____________________________________________. Complete this section only if you are reporting a loss of income. Date employment ended | fecha que el empleo terminó? If hours/rate of pay has varied, please explain. In order to determine the eligibility of ___________________________________________ for public assistance, please assist us by.

2002 Form FL DCF CFES 2620 Fill Online, Printable, Fillable, Blank
In order to determine the eligibility of ___________________________________________ for public assistance, please assist us by. Verification of employment/loss of income in order to determine the eligibility of _____________________________________________. Date employment ended | fecha que el empleo terminó? Complete this section only if you are reporting a loss of income. If hours/rate of pay has varied, please explain.
Verification Of Employment Loss PDF Form FormsPal
Complete this section only if you are reporting a loss of income. Verification of employment/loss of income in order to determine the eligibility of _____________________________________________. In order to determine the eligibility of ___________________________________________ for public assistance, please assist us by. If hours/rate of pay has varied, please explain. Date employment ended | fecha que el empleo terminó?
Self employed loss of letter Fill out & sign online DocHub
In order to determine the eligibility of ___________________________________________ for public assistance, please assist us by. If hours/rate of pay has varied, please explain. Verification of employment/loss of income in order to determine the eligibility of _____________________________________________. Date employment ended | fecha que el empleo terminó? Complete this section only if you are reporting a loss of income.
Fillable Online loss of verification form Fax Email Print
Complete this section only if you are reporting a loss of income. Verification of employment/loss of income in order to determine the eligibility of _____________________________________________. Date employment ended | fecha que el empleo terminó? If hours/rate of pay has varied, please explain. In order to determine the eligibility of ___________________________________________ for public assistance, please assist us by.

Address To Verification Of Employment Loss Of Form Florida
If hours/rate of pay has varied, please explain. In order to determine the eligibility of ___________________________________________ for public assistance, please assist us by. Complete this section only if you are reporting a loss of income. Verification of employment/loss of income in order to determine the eligibility of _____________________________________________. Date employment ended | fecha que el empleo terminó?
FREE 9+ Sample Verification Forms in PDF MS Word
In order to determine the eligibility of ___________________________________________ for public assistance, please assist us by. Complete this section only if you are reporting a loss of income. Verification of employment/loss of income in order to determine the eligibility of _____________________________________________. If hours/rate of pay has varied, please explain. Date employment ended | fecha que el empleo terminó?
Complete This Section Only If You Are Reporting A Loss Of Income.
Verification of employment/loss of income in order to determine the eligibility of _____________________________________________. Date employment ended | fecha que el empleo terminó? If hours/rate of pay has varied, please explain. In order to determine the eligibility of ___________________________________________ for public assistance, please assist us by.