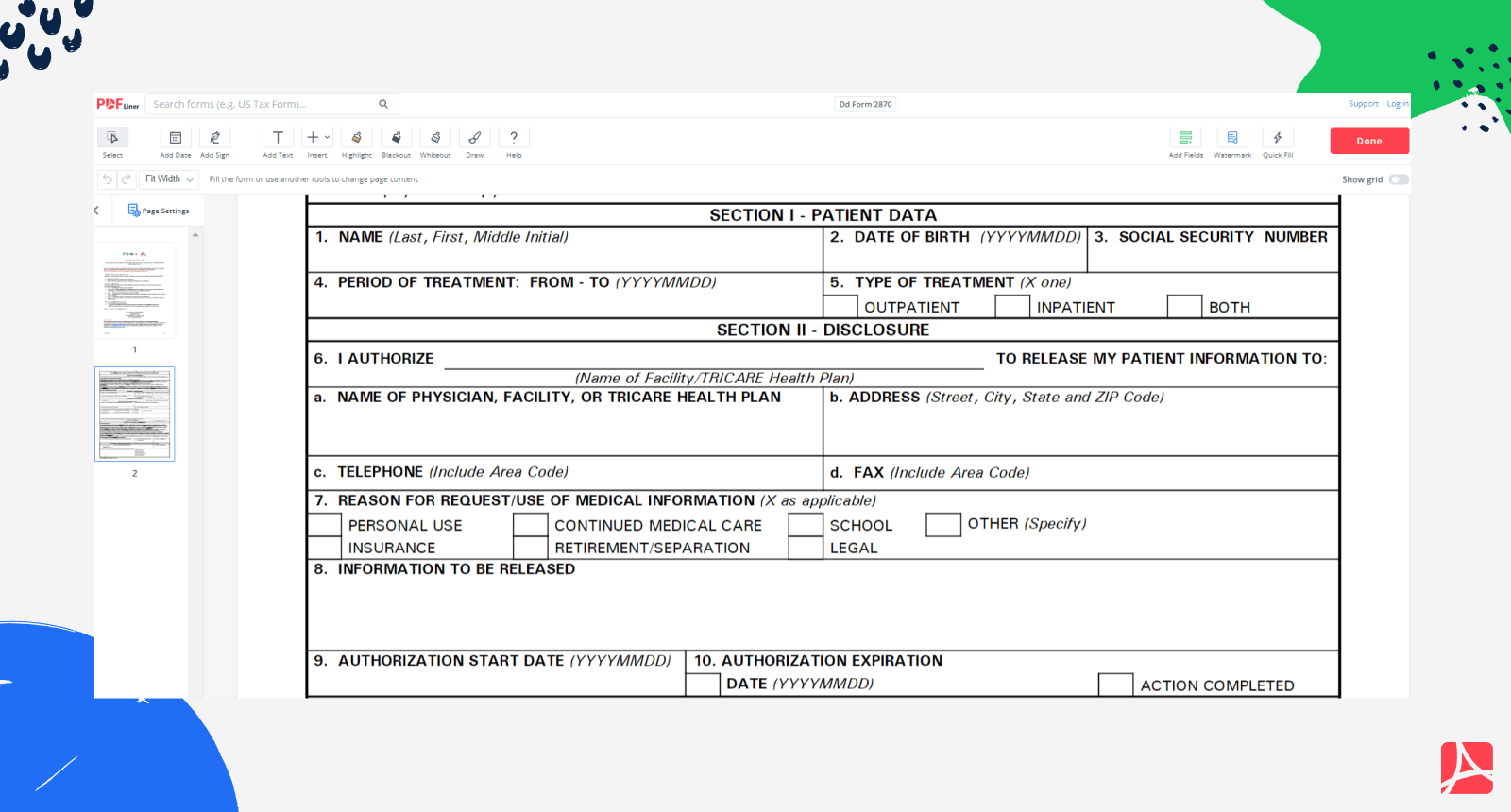
Dd Form 2870 Release Of Information - This form will not be used for the authorization to disclose. The attached dd form 2870, authorization for disclosure of medical or dental information, authorizes fox army health center (fach) to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to request the use and/or. Full name in (last, first, middle initial) format block 2: Date of birth in (yyyymmdd) format block 3: This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to. (dd form 2870) this form is used to allow a tricare beneficiary to authorize health net federal services, llc (health net) to. Dd form 2870 instructions block 1:
This form will not be used for the authorization to disclose. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to. Full name in (last, first, middle initial) format block 2: Dd form 2870 instructions block 1: Date of birth in (yyyymmdd) format block 3: The attached dd form 2870, authorization for disclosure of medical or dental information, authorizes fox army health center (fach) to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to request the use and/or. (dd form 2870) this form is used to allow a tricare beneficiary to authorize health net federal services, llc (health net) to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to.
This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to. The attached dd form 2870, authorization for disclosure of medical or dental information, authorizes fox army health center (fach) to. This form will not be used for the authorization to disclose. Full name in (last, first, middle initial) format block 2: Date of birth in (yyyymmdd) format block 3: This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to. (dd form 2870) this form is used to allow a tricare beneficiary to authorize health net federal services, llc (health net) to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to request the use and/or. Dd form 2870 instructions block 1:

DD Form 2870 Authorization for Disclosure of Medical or Dental Information
This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to request the use and/or. Dd form 2870 instructions block 1: (dd form 2870) this form is used to allow a tricare beneficiary to authorize health net.

DD Form 2870 Online Dental, Medical, Information privacy
This form will not be used for the authorization to disclose. (dd form 2870) this form is used to allow a tricare beneficiary to authorize health net federal services, llc (health net) to. Dd form 2870 instructions block 1: The attached dd form 2870, authorization for disclosure of medical or dental information, authorizes fox army health center (fach) to. This.
DD Form 2870 Printable Dd Form 2870 blank, sign online — PDFliner
The attached dd form 2870, authorization for disclosure of medical or dental information, authorizes fox army health center (fach) to. Full name in (last, first, middle initial) format block 2: This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to request the use and/or. Date of birth in (yyyymmdd) format block 3: This.

Fillable Online benning army DD Form 2870 Authorization for Disclosure
The attached dd form 2870, authorization for disclosure of medical or dental information, authorizes fox army health center (fach) to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to. This form is to provide the.

Dd Form 2870 Fill out Printable PDF and Word Sample
This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to. This form will not be used for the authorization to disclose. Full name in (last, first, middle initial) format block 2: (dd form 2870) this form.

Fillable Online Instructions for Completing the DD Form 2870
(dd form 2870) this form is used to allow a tricare beneficiary to authorize health net federal services, llc (health net) to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to request the use and/or..
Dd Form Army Fillable Fill Online Printable Fillable Blank sexiezpix
The attached dd form 2870, authorization for disclosure of medical or dental information, authorizes fox army health center (fach) to. This form will not be used for the authorization to disclose. Full name in (last, first, middle initial) format block 2: (dd form 2870) this form is used to allow a tricare beneficiary to authorize health net federal services, llc.

Free clip dd 2870 form, Download Free clip dd 2870 form png images
Date of birth in (yyyymmdd) format block 3: Full name in (last, first, middle initial) format block 2: The attached dd form 2870, authorization for disclosure of medical or dental information, authorizes fox army health center (fach) to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to request the use and/or. (dd.
Dd form 2870 Fill out & sign online DocHub
Date of birth in (yyyymmdd) format block 3: (dd form 2870) this form is used to allow a tricare beneficiary to authorize health net federal services, llc (health net) to. The attached dd form 2870, authorization for disclosure of medical or dental information, authorizes fox army health center (fach) to. Full name in (last, first, middle initial) format block 2:.

DD Form 2870 Authorization for Disclosure of Medical or Dental Information
The attached dd form 2870, authorization for disclosure of medical or dental information, authorizes fox army health center (fach) to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to. Dd form 2870 instructions block 1: This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to..
Full Name In (Last, First, Middle Initial) Format Block 2:
The attached dd form 2870, authorization for disclosure of medical or dental information, authorizes fox army health center (fach) to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to. This form is to provide the military treatment facility/dental treatment facility/tricare health plan with a means to request the use and/or.
Dd Form 2870 Instructions Block 1:
This form will not be used for the authorization to disclose. Date of birth in (yyyymmdd) format block 3: (dd form 2870) this form is used to allow a tricare beneficiary to authorize health net federal services, llc (health net) to.